ETS Reversal Information
Dr.Reisfeld does perform reversal operations. The type of reversal is dependent on the type of surgery initially performed (the cutting of the nerve, versus the clamping of it).
Over the last decade, more and more ETS surgeries have been performed. Before about 1990, all of the sympathectomies were done in an open fashion that neither physicians or patients preferred. The endoscopic approach made it easier for patients and surgeons alike to accept the operation. It is primarily used for problems like excessive sweaty hands, facial blushing, and facial sweating. The term hypersympathetic activity is used to describe this condition as a physiological manifestation of a hyperactive sympathetic system.
Another reason why more ETS procedures have been done over the last decade, is due to the recent increase and quality of information available on the internet. The dramatic increase in the number of cases being done also brought with it a certain amount of patients (about 3% to 5%) who are unhappy with the results.
For those patients who are unhappy with the results of the surgery, there is a solution. In the past, the only method that was done endoscopically, was the cutting method. For those cases, an attempt was made with some medications, but when that failed then the reversal operations was next. It involved a nerve graft. More recently, the clamping method has also been used, making the reversal operation easier (simply removing the clips). Below, both types of reversals that Dr. Reisfeld has performed in the past are reviewed.
Nerve Graft
With this method, a nerve graft is taken from the ankle region (the sural nerve), and is connected to the divided edges of the sympathetic chain. This is done with a special biological glue. The operation has two components:
- Mechanical
- Physiological
Mechanical (Surgery)
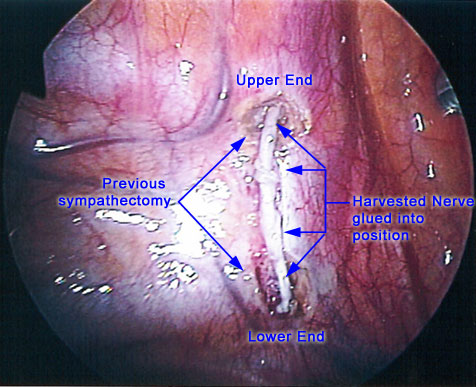
The mechanical portion is composed of an endoscopic approach to the prior sympathectomy site (the location where the operation was previously done). The surgeon refreshes the edges of the previously cut nerve. This can be done with an ultrasound scalpel, or with scissors not connected to electricity.
This part is not always possible due to severe scar tissue that builds up during the initial operation. In cases where severe scar tissue is found, the operation may be aborted. Also, any other technical difficulties can terminate the attempt, although this is not common.
Once the area of the previous sympathectomy is prepared, the intercostal nerve graft, or any other nerve graft, is sutured or glued to the missing segment and the procedure is finished. The same procedure is performed on the other side of the chest cavity.
Physiological
(Time it takes for the nerve itself to resume conduction)
In this second portion, the time needed for the nerve to return to normal sympathetic regulation is a matter that is different from one patient to another. The amount of information that we have about it is very minimal. The process can take a long time, and initial symptoms of recovery will not always show before 6 to 9 months after the reversal.
So far, cases done by Dr. Reisfeld show some improvement. The improvements can be seen in a lessening of compensatory sweating, a better ability to perform exercises, a return of sweat to the facial area and upper body, and better cooling of the upper body regions. These results are similar to those reported by Dr. Telaranta, who also does this reversal.
At a meeting in Germany (2003), the results of nerve graft reversal were presented by Dr. Reisfeld and Dr. Telerantra. Both surgeons reported similar results, however, there is a long way to go in order to get definitive statistical data. In order to get meaningful data, we will need to perform many more cases with a longer followup.
Similar work for nerve graft reversal is being done by urological physicians (plastic surgeons who use the sural nerve to repair damage done to the sympathetic chain within the pelvic cavity). Here, the sural nerve graft is used as a tube similar to what is done in our reversal procedure. The difference is that they do it immediately at the time of the initial operation.
This other procedure is done in an open fashion with very fine sutures. Their results are not yet etched in stone, and in a recent verbal communication with the leading plastic surgeon who performs these operations, the need for more cases and longer followup was emphasized.
One clear fact, is that the shorter the segment that is cut the better the chances are for reversibility with the nerve graft. There are too few cases to really say anything more than this for now.
Intercostal Nerve Graft
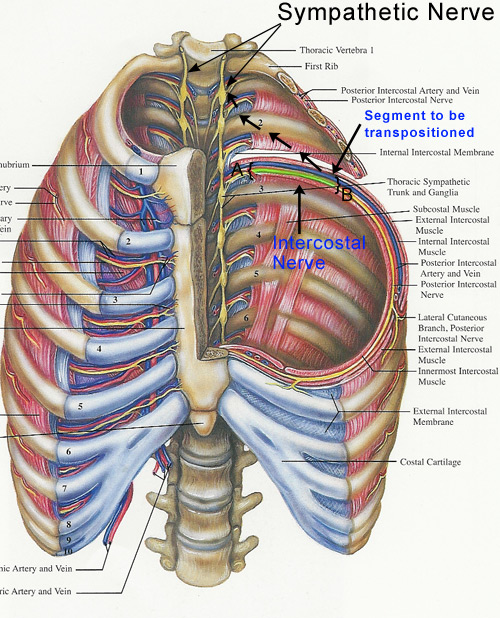
In regards to the intercostals nerve graft method, please refer to the picture below and notice the complex and unique method that can be used to bridge the segment that was taken off in the original ETS surgery.
-
- The difficulties that a surgeon might encounter when performing the intercostals nerve graft procedure are few. Among them, are the length of the segment that was taken, and the amount of scar tissue that might be found during the initial exploration.
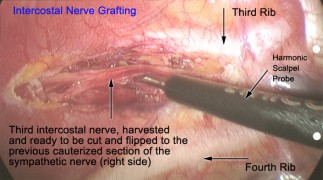
- In the picture (open diagram), one can see a harvested intercostal nerve at the third rib level. This was harvested and freed from the surrounding tissues and flipped over to the site of the previously divided sympathetic nerve. The theoretical benefit of this intercostal nerve graft, is that the blood supply is maintained to the harvested nerve. The intercostal nerve also contains some sympathetic and sensory fibers, which might add to the physiological response. Again, with this method more cases have to be done, and more follow-up is needed.
- As equipment and technical dexterity improves, it is now possible to perform the intercostal grafting procedure with very fine sutures to connect the end of the graft. With this technique, a there is a better chance of recovery. Both methods that are now used are done with robotic equipment or modern refined endoscopic equipment.
- As said in the previous paragraph, the incorporation of suturing in order to bring the nerve ends together is much more effective and promising. More cases are needed to provide a definite statement. Situations where numbness in the chest wall where the nerve was used is now better understood, but further follow-ups are required to understand this rare occurrence.
This is a very complex procedure, so let’s review:
-
- The harvested intercostal nerve has a limited length that can be used to connect the lower part of the sympathetic chain to the upper part that was cut. If a patient had more than 2-3 levels that were cut, the amount of nerve available might not be enough for a successful connection. Obviously This decision not to move forward can be done only after a long time is spent in the operating room to determine if you they have the appropriate measurements. No pre-operative decisions can be made before an actual operation, thus complicating the matter even further.
- If the previous ETS procedure was done at a high level (T2-T3), it makes the preparation of the upper end of the sympathetic chain too close to the stellate ganglion to enable a safe connection. This could also potentially cause Horner’s syndrome if the procedure is performed. Because of the limited number of cases done, and the fact that the success rate is yet to be established, it is better not to risk this permanent complication. You should discuss this type of procedure with your surgeon before moving forward.
Reversal Using The Clamping Method
Since about 1999, the clamping method has became the method of choice for Dr. Reisfeld. Dr. Reisfeld only does the clamping method for his patients. If a patient is unhappy with the results, the clamps can be taken out, giving the patient more potential for reversal and recovery.
So far, Dr. Reisfeld has performed several clamp removal reversals. those cases have shown improvement in compensatory sweating (compensatory hydrosis or reflex sweating), and performance ability. The healing process and improvement of the symptoms can take up to a year.
Dr. Reisfeld wishes to emphasize that the clamping method does not guarantee complete reversal. He simply believes that the clamping method offers the best chances of recovery.
As time goes by, more cases will be done and more information will be gathered. Those results and experiences will be posted as soon as they are available. For the time being, about 37 reversal cases have been done on patients who previously had the clamping method. About half of them show improvement.
The improvement presents itself with a reduction of compensatory sweating, return of sweat to the facial region, and minimal to mild hand sweating. As more time has passed, we are getting more and more patients who indeed testify that the clamp removal reduced or eliminated their side effects. In some of those cases it took 2 to 3 years to see the benefits from clamp removal. This fact is in line with the knowledge that nerve growth and recovery of the autonomous nervous system is a very slow process.
Recently, an unpublished medical paper described the experience of European surgeons that described the results of clamp removal over 10 years. It reflects the opinion of Dr. Reisfeld, that the clamp removal does have positive results over time. One should bear in mind that it is a very complicated matter, and not all the facts are yet known to us. The sympathetic chain is still a very unknown entity in neurological science.
A lot has yet to be explored. We know that it has some sort of regeneration ability, but to what degree is still a mystery. We can draw clinical experience through statements, but again those are not always consistent. The fact is that some cases showed recovery after clip removal, which was primarily a factor of time but not always.
Also one should bear in mind that compensatory sweating is something that changes with time, even without clip removal. If a patient wishes to have their clamps removed, they should speak to their surgeon.
Do you have any questions that were not answered here? Would you like to speak with Dr. Reisfeld to answer those questions? To learn more about what we can do for you, contact The Center for Hyperhidrosis by contacting our office.